

Severs Heel Pain – What Is It?
Severs, which is also known as calcaneal apophysitis (calcaneum is the heel bone), was first described by American Orthopaedic Surgeon James Warren Sever in 1912 and is considered inflammation of the growth plate in the heel of growing children (1). As children are growing, their bones are considered to not be ‘fully developed’.
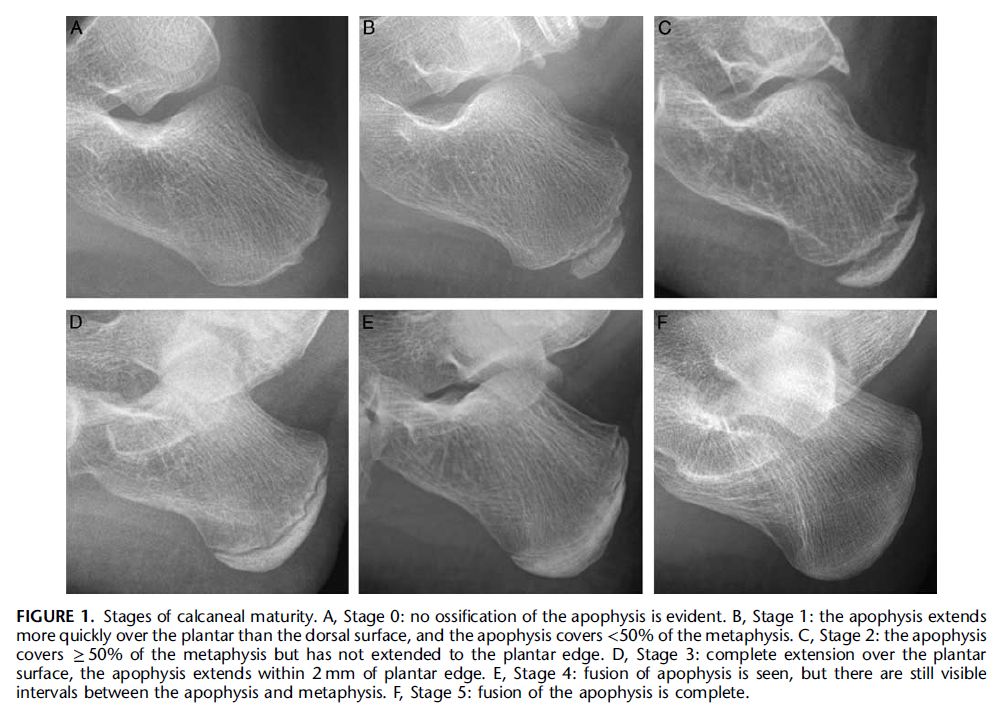
The growth plate at the heel starts it’s forming process at the average age of 7.2 years for females and 9.64 for males. See the x-ray pictures below to see the development from no formation of the growth plate at Stage 0 to full fusion of the growth plate at Stage 5. Stage 5 begins its process towards full fusion at average age of 13.44 for females and 15.24 for males (2).
Severs heel pain commonly occurs between the ages of 8 and 15 years of age (2) particularly in those involved in running and jumping activities during the pubertal growth spurt (3). In 30% of cases Severs heel pain is experienced in both heels (1).
It is speculated to be an “overuse injury” in children and adolescents (2) involving repetitive microtrauma of the achilles tendon (3). The achilles tendon transmits force to where it attaches at the heel and growth plate region due to repeated calf muscle contraction associated with playing sport and being highly active (3).
Research has shown that there was an on average pain duration of 10.8 months prior to seeking medical intervention. The authors believe this may be due to the difference between children’s scoring and their parents scoring of physical function level related to the heel pain. Children score higher in the initial periods of experiencing heel pain when compared to their parents scoring of their children’s physical levels.
What might an assessment from a physiotherapist include for a child or teenager with heel pain?
A physical assessment looking at ankle range of motion, foot and ankle muscle strength and stability, balance/proprioception is likely to be included. A ‘squeeze test’ to determine pain to press around the region of the growth plate of the heel can help the clinician ascertain as to whether Severs is the diagnosis. Provided prior trauma to the heel and ankle region is excluded, as well as any other pathology to the area is ruled out; x-ray or other radiographic scan is typically not necessary to aid a diagnosis of Severs (4).
What can be done about it?
Severs heel pain often fully resolves once the heel bone has completed growth (see Stage 6 in the above picture) or when activities reduces (1). Decreasing aggravating activities such as running and jumping can assist in the reduction of symptoms (1).
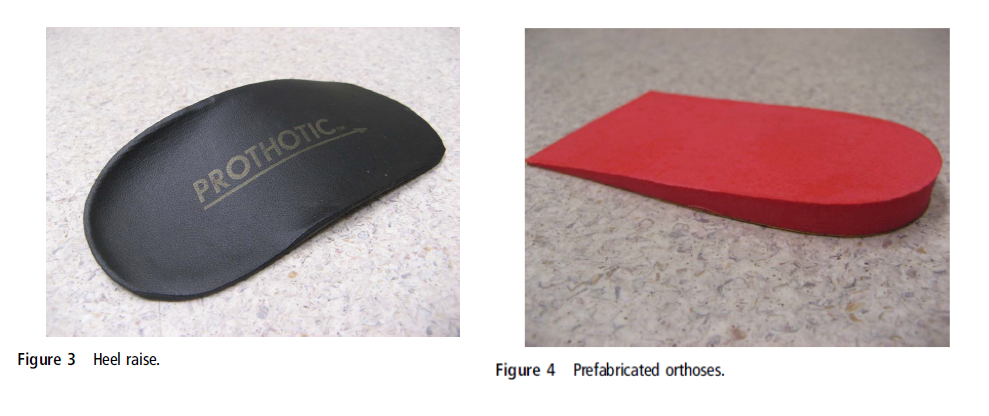
Currently there is limited high quality research investigating interventions to help decrease Severs heel pain (5). One study compared the input of a heel raise to a prefabricated orthotic in children with Severs (all children were instructed to ice their painful heel/s 10 minutes per day and perform calf muscle stretching) (see images below) (6). The heel raises were considered to be more beneficial than the prefabricated orthotic early on in to the treatment period (at 1 and 2 month points) but no different later on (at 6 and 12 month time points).
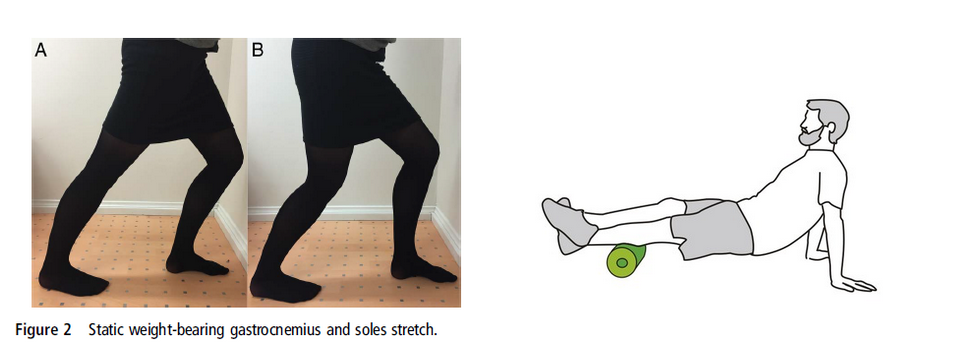
Despite a lack of research evidence investigating it’s use; stretching and foam rolling (self-massage) of the calf muscles to improve ankle (dorsiflexion) range of motion may be considered in those with Severs heel pain. Soft tissue massage from a physiotherapist may also be considered with aim help relieve heel symptoms.
Consideration of a heel raise in to the shoe to off-load the heel or a shoe insert (orthotic) may also be options to discuss with a physiotherapist or podiatrist.
How can I prevent this from developing?
A common time that physiotherapist’s see children and adolescents for this condition is in pre-seasons of sport where there is a rapid increase in activity levels (running and jumping) after a period of reduced activity (e.g. return to pre-season training following the December/January holiday period). Minimising spikes in activity levels can help minimise risk of Severs heel pain developing.
Jogging requires 6 times your bodyweight each step. One of the calf muscles, the gastrocnemius produces 3 times your bodyweight of force each step when jogging and the other calf muscle soleus produces 8 times your bodyweight of force each step. Increasing calf muscle strength/endurance capacity may reduce the load through the heel region and possibly minimising risk of heel pain developing. Performing heel raises (double leg and/or single leg heel raises) twice per week would be a good option to help reduce risk.
In addition, ensuring good flexibility at the ankle with regular calf muscle stretching can help improve ankle (dorsiflexion) range of motion. Performing calf stretching with a bent knee and straight leg are good options.
In summary, Severs heel pain is a common condition seen in children and adolescents as the growth plate in the heel is developing and fusing. Severs heel pain is often related to rapid increases in running and jumping activity. Strategies such as monitoring physical activity levels, increasing calf muscle strength and improve ankle range of motion may help minimise this condition from occurring.
- Agyekum, E. K., & Ma, K. (2015). Heel pain: A systematic review. Chinese Journal of Traumatology, 18(3), 164-169.
- Duong, M. M., Nicholson, A. D., Li, S. Q., Gilmore, A., Cooperman, D. R., & Liu, R. W. (2018). Relationship Between Sever Disease and Skeletal Maturity. Journal of pediatric orthopedics.
- Davison, M. J., David-West, S. K., & Duncan, R. (2016). Careful assessment the key to diagnosing adolescent heel pain. The Practitioner, 260(1793), 30-2
- Kose, O. (2010). Do we really need radiographic assessment for the diagnosis of non-specific heel pain (calcaneal apophysitis) in children?. Skeletal radiology, 39(4), 359-361.
- James, A. M., Williams, C. M., & Haines, T. P. (2013). Effectiveness of interventions in reducing pain and maintaining physical activity in children and adolescents with calcaneal apophysitis (Sever’s disease): a systematic review. Journal of foot and ankle research, 6(1), 16.
- James, A., Williams, C., & Haines, T. (2016). Effectiveness of footwear and foot orthoses for calcaneal apophysitis: A 12-month factorial randomised trial. British Journal of Sports Medicine,50(20), 1268-1275.