

What is Causing My Shoulder and Arm Pain? Part 1: The Rotator Cuff.
Shoulder Pain has been shown to significantly affect people’s Quality of Life. A recent study found that of a group of 384 people; shoulder pain had the MOST impact on physical AND mental quality of life; when compared to low back pain, sciatica and knee pain (1).
Shoulder pain is the 3rd most common musculoskeletal problem presenting to Australian GP’s only behind back pain and knee pain (2).
Some studies have shown as high as up to 67% of people will experience shoulder pain at some point throughout their life (lifetime prevalence) (3). Up to 34% of people aged >65 experience shoulder pain (point prevalence) (3).
40-50% of new shoulder pain presentations continue to experience symptoms 6-12 months after onset (3,4). The rotator cuff is the most commonly affected structure, involved in roughly 65-70% of all shoulder presentations (5).
What is the Rotator Cuff?
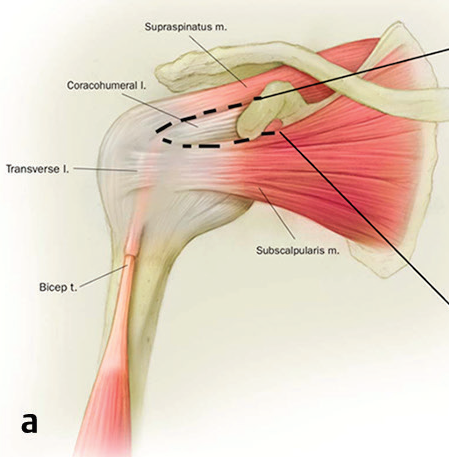
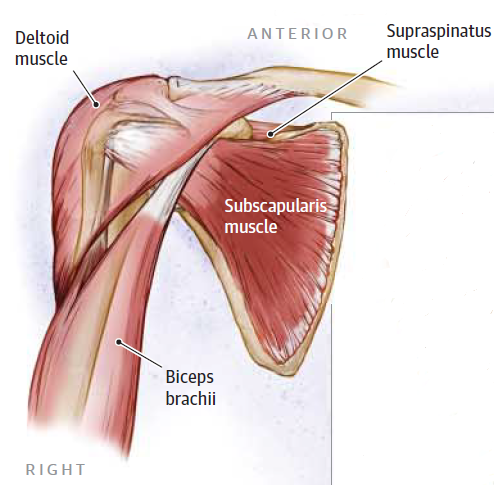
There are 4 muscles that make up the rotator cuff. The tendons of these 4 muscles share common attachments from the shoulder blade (scapula) to the ball of this ball-and-socket shoulder joint. See the picture below showing these 4 rotator cuff muscles named the supraspinatus, subscapularis, infraspinatus and teres minor (6). The rotator cuff muscles help provide both stability and movement of the ball-and-socket joint.
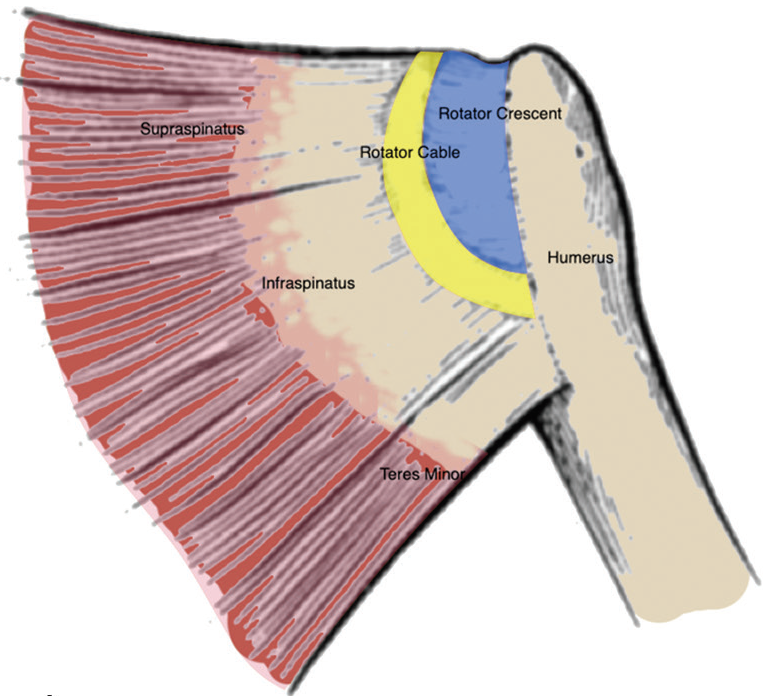
Picture on right – view from behind right shoulder showing Supraspinatus, Infraspinatus and Teres Minor muscles. (6)
Several different names have been given for what Dr. Jeremy Lewis has coined Rotator Cuff Related Shoulder Pain (7). This name encompasses the various rotator cuff tendons and surrounding bursa (sac of fluid preventing friction between tendon and bone). The common names you may have heard from your GP, a physio, medical practitioner or friend with shoulder symptoms include;
- Rotator cuff tendinopathy/tendinosis
- Supraspinatus tendinitis/tendinopathy/tendinosis
- Partial/Full Thickness Rotator Cuff Tear
- Subacromial Bursitis
- Subacromial Impingement Syndrome
- Shoulder Impingement Syndrome
- Subacromial Pain Syndrome
- Shoulder Pain Syndrome

Who Is At Risk Of A Rotator Cuff Tear?
1. Age
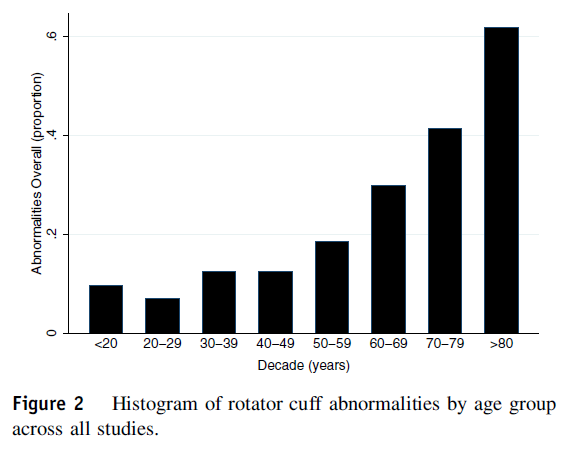
A systematic review looked at several studies that performed radiology scans of the shoulder in people with and without shoulder pain (10)
- See the graph below showing with each decade of life the prevalence of people shown to have rotator cuff tears (10).
- 19% of those aged 50-59 years were shown to have a rotator cuff tear.
- 9.5% of those aged 50-59 with no shoulder symptoms had a rotator cuff tear.
- 30% of those aged 60-69 years were shown to have a rotator cuff tear.
- 16% of those aged 60-69 years with no shoulder symptoms had a rotator cuff tear.
- 41% of those aged 70-79 years were shown to have a rotator cuff tear.
- 28% of those aged 70-79 years with no shoulder symptoms had a rotator cuff tear.
- 62% of those aged 80-89 years were shown to have a rotator cuff tear.
- 56% of those aged 80-89 years with no shoulder symptoms had a rotator cuff tear.
- The number of those people with rotator cuff tears experiencing no symptoms suggests a tear does not always result in pain.
- Another Systematic Review found age greater than 50 years of age to be a key risk factor for developing rotator cuff tendon pain (tendinopathy) (11)
2. Type 2 Diabetes
A strong link was shown between those with Type 2 Diabetes and their risk of Tendon Rupture (their risk of injuring all types of tendon tissue in the body were higher) (12)

3. Overhead Shoulder Activity (greater than 90 degrees elevation)
- Those shown to work in positions where the arm is elevated above 90 degrees (shoulder height) for sustained periods reported higher levels of shoulder complaints of pain and disability (11,14). This was seen in House Painters when compared to Machine Operators and Car Mechanics (14).
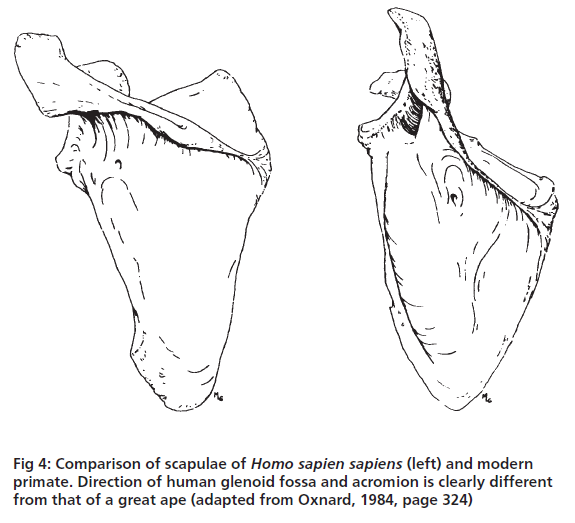
- See below the comparison of the human scapula (shoulder blade) (on the left) compared to that of an ape (on the right) (15). The socket (glenoid) of the ape is more upward facing whereas the human’s glenoid (socket) is more laterally facing. Ape’s and chimpanzee’s ability to swing overhead (brachiate) is much superior to the human and this is one of the suggested reasons why. This implies that human’s may have more difficulty with overhead movement and particular sustained positions above 90 degrees as our anatomy is less suited to prolonged overhead activity. In addition, it has been suggested that the supraspinatus muscle has become smaller over time suggesting it is working relatively harder in the modern shoulder girdle and may predispose it to “overuse and breakdown” of this rotator cuff muscle/tendon possibly subjecting it to higher chance of injury (15).
Overhead Sport
State, national and international swimmers based in Victoria were followed throughout a 12 month period. A high incidence rate of up to 38% of swimmers experienced a shoulder injury in this 12 month period. Interestingly, the main factors associated with shoulder injury was either too much or too little (external rotation) range of motion (>100 degrees or <93 degrees). Additionally a previous history of shoulder pain in the swimming athlete was another risk factor for developing shoulder pain. The amount of kilometres swum in this study was not a risk factor but considering the large volumes of repetitive overhead motions with the above history may increase the chance of developing shoulder symptoms (16)
- Sports with higher incidence of overuse shoulder injuries in youth athletes were tennis, baseball and volleyball all requiring repetitive overhead motion (17)
- The incidence of shoulder injuries for all age groups as high as 17% (18).

4. History of Trauma
- One third (33.5%) of those with a history of shoulder dislocation were shown to have rotator cuff tears (10)
- A survey investigating possible risk factors in those with and without shoulder pain found that a history of trauma was shown to significantly correlate with rotator cuff tear (19)
5. External Rotation Strength
Reduced External Rotation Strength was shown to be a risk factor for developing shoulder pain in elite male handball players (20). When testing external rotation strength this is looking at strength of the rotator cuff muscles suggesting weakness to these muscles may predispose someone to shoulder injury.

Rotator cuff tears are a commonly experienced musculoskeletal injury affecting people’s quality of life (1). Over the coming days we will provide further information regarding treatment options for shoulder pain.
Are you experiencing shoulder and/or arm pain? Wondering what to do about it?
Click on the link below to book your Free 15 Minute Phone Call and we would be happy to talk with you about your problem to determine if we can be of help.
References:
- Imagama, S., Ando, K., Kobayashi, K., Seki, T., Hamada, T., Machino, M., . . . Hasegawa, Y. (2020). Shoulder pain has most impact on poor quality of life among various types of musculoskeletal pain in middle-aged and elderly people: Yakumo study. Modern Rheumatology, 30(3), 568-572.
- Britt H, Miller GC, Charles J, Henderson J, Bayram C, Pan Y, Valenti L, Harrison C, O’Halloran J & Fahridin S 2010. General practice activity in Australia 2009–10. General practice series no. 27. Cat. no. GEP 27. Canberra: AIHW.
- Luime, J., Koes, B., Hendriksen, I., Burdorf, A., Verhagen, A., Miedema, H., & Verhaar, J. (2004). Prevalence and incidence of shoulder pain in the general population; a systematic review. Scandinavian Journal of Rheumatology, 33(2), 73-81.
- Ottenheijm, R., Joore, M., Walenkamp, G., Weijers, R., Winkens, B., Cals, J., . . . Dinant, G. (2011). The Maastricht Ultrasound Shoulder pain trial (MUST): Ultrasound imaging as a diagnostic triage tool to improve management of patients with non-chronic shoulder pain in primary care. BMC Musculoskeletal Disorders, 12(1), 154.
- Edwards, P., Ebert, J., Joss, B., Bhabra, G., Ackland, T., & Wang, A. (2016). EXERCISE REHABILITATION IN THE NON-OPERATIVE MANAGEMENT OF ROTATOR CUFF TEARS: A REVIEW OF THE LITERATURE. International Journal of Sports Physical Therapy, 11(2), 279-301.
- Asghar, A., Ghosh, S., & Narayan, R. (2020). Revisiting the Anatomy of Rotator Cuff Relevant to Rotator Cuff Injury. National Journal of Clinical Anatomy, 9(1), 01-06.
- Lewis, J. (2016). Rotator cuff related shoulder pain: Assessment, management and uncertainties. Manual Therapy, 23, 57-68.
- Littlewood, C., & Cools, A. (2018). Scapular dyskinesis and shoulder pain: The devil is in the detail. British Journal of Sports Medicine, 52(2), 72-73.
- Minagawa, H., Yamamoto, N., Abe, H., Fukuda, M., Seki, N., Kikuchi, K., . . . Itoi, E. (2013). Prevalence of symptomatic and asymptomatic rotator cuff tears in the general population: From mass-screening in one village. Journal of Orthopaedics, 10(1), 8-12.
- Teunis, Teun, MD, Lubberts, Bart, BSc, Reilly, Brian T., BSc, & Ring, David, MD, PhD. (2014). A systematic review and pooled analysis of the prevalence of rotator cuff disease with increasing age. Journal of Shoulder and Elbow Surgery, 23(12), 1913-1921.
- Leong, H., Fu, S., He, X., Oh, J., Yamamoto, N., & Yung, S. (2019). Risk factors for rotator cuff tendinopathy: A systematic review and meta-analysis. Journal of Rehabilitation Medicine, 51(9), 627-637.
- Zakaria, M., Davis, W., & Davis, T. (2014). Incidence and predictors of hospitalization for tendon rupture in Type 2 diabetes: The Fremantle Diabetes Study. Diabetic Medicine, 31(4), 425-430.
- Hermans, J., Luime, J., Meuffels, D., Reijman, M., Simel, D., & Bierma-Zeinstra, S. (2013). Does This Patient With Shoulder Pain Have Rotator Cuff Disease?: The Rational Clinical Examination Systematic Review. JAMA : The Journal of the American Medical Association, 310(8), 837-847.
- Svendsen, S., Bonde, J., Mathiassen, S., Stengaard-Pedersen, K., & Frich, L. (2004). Work related shoulder disorders: Quantitative exposure-response relations with reference to arm posture. Occupational and Environmental Medicine (London, England), 61(10), 844-853.
- Lewis, J., Green, A., Yizhat, Z., & Pennington, D. (2001). Subacromial impingement syndrome: Has evolution failed us? Physiotherapy, 87(4), 191-198.
- Walker, H., Gabbe, B., Wajswelner, H., Blanch, P., & Bennell, K. (2012). Shoulder pain in swimmers: A 12-month prospective cohort study of incidence and risk factors. Physical Therapy in Sport, 13(4), 243-249.
- Kraan, R., De Nobel, D., Eygendaal, D., Daams, J., Kuijer, P., & Maas, M. (2019). Incidence, prevalence, and risk factors for elbow and shoulder overuse injuries in youth athletes: A systematic review. Translational Sports Medicine, 2(4), 186-195.
- Abrams, G., Renstrom, P., & Safran, M. (2012). Epidemiology of musculoskeletal injury in the tennis player. British Journal of Sports Medicine, 46(7), 492-498.
- Yamamoto, Atsushi, MD, Takagishi, Kenji, MD, PhD, Osawa, Toshihisa, MD, PhD, Yanagawa, Takashi, MD, PhD, Nakajima, Daisuke, MD, Shitara, Hitoshi, MD, & Kobayashi, Tsutomu, MD, PhD. (2010). Prevalence and risk factors of a rotator cuff tear in the general population. Journal of Shoulder and Elbow Surgery, 19(1), 116-120.
- Clarsen, B., Bahr, R., Andersson, S., Munk, R., & Myklebust, G. (2014). Reduced glenohumeral rotation, external rotation weakness and scapular dyskinesis are risk factors for shoulder injuries among elite male handball players: A prospective cohort study. British Journal of Sports Medicine, 48(17), 1327-1333.